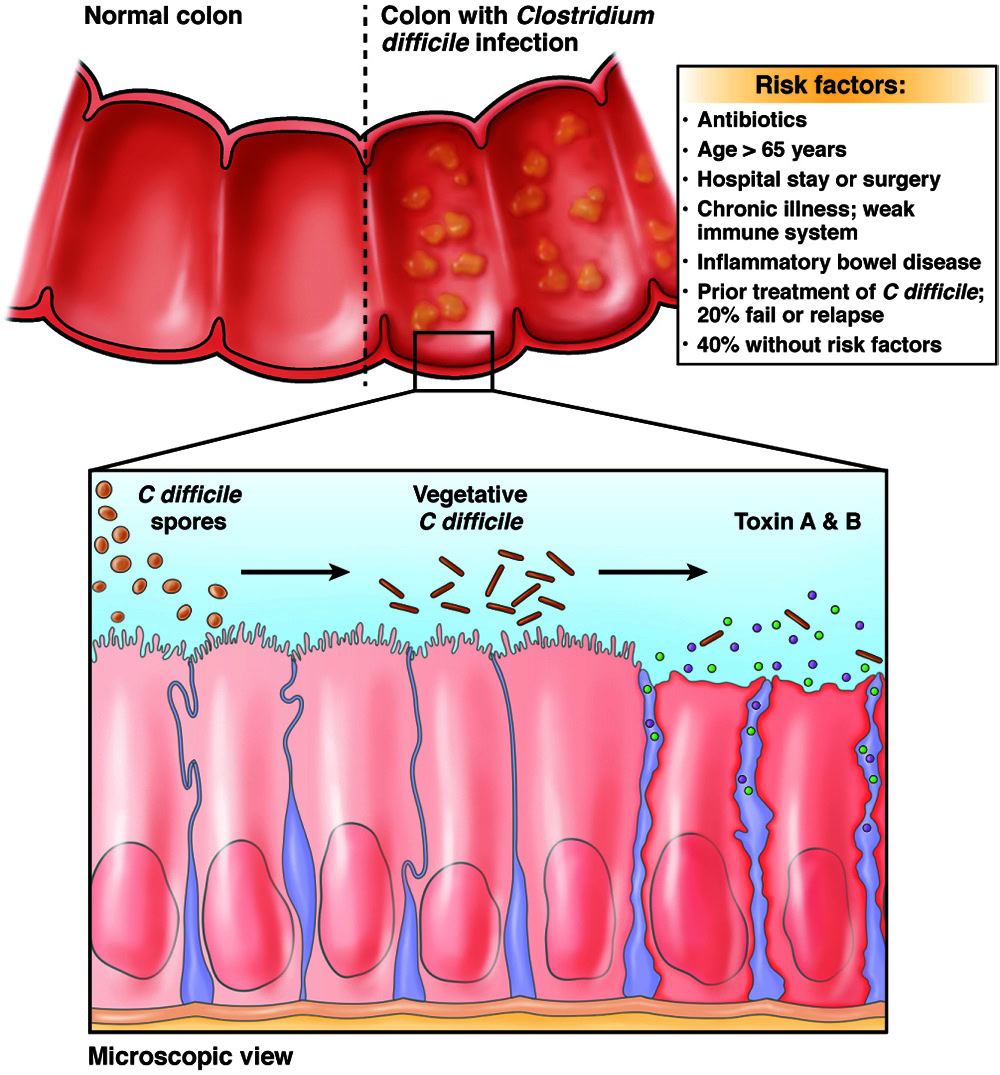
What is C. diff?
Clostridioides difficile (previously known as Clostridium difficile), or C. diff for short, is an infection from a bacterium that can grow in your intestines and cause bad GI symptoms.
Each year, C. diff infects roughly 375,000 people in the U.S. and often calls for hospitalization. The main risk of getting C. diff infection is antibiotic use.

Things to know about C. diff:
- C. diff is very contagious.
- C. diff can usually be treated with antibiotics, but sometimes additional treatments are needed to get rid of the infection.
- Unlike other intestinal bacteria, it can take a long time to get rid of C. diff and start feeling better.
- In very bad cases, C. diff infection can be deadly, with estimates of C. diff-linked death ranging from 14,000 to 30,000 each year.
C. diff and IBD
Empowering you with information from the latest AGA Clinical Practice Update (Khanna et al., 2026)
People with inflammatory bowel disease (IBD, Crohn’s disease or ulcerative colitis) are at a higher risk of getting C. diff than people without IBD. About 1 in 10 hospitalized patients with IBD may develop C. diff. Almost 3 out of 10 patients with IBD and diarrhea may be diagnosed with C. diff.
C. diff can trigger flares, lead to hospitalization, make IBD treatments less effective, and increase the risk of surgery. Symptoms of C. diff and an IBD flare can look the same, so talking to your health care provider about testing and treatment options is important.
C. diff and IBD symptoms
If you have IBD and develop new or worsening diarrhea, always ask your care team: “Have we ruled out C. diff?”
Any new or worse diarrhea in patients with IBD should prompt stool testing for C. diff, even if:
- You haven’t taken antibiotics recently.
- You think it’s “just a flare.”
This includes people with an ostomy or J-pouch who notice higher output.
Alarm symptoms
Severe symptoms need urgent care. Seek immediate care if you have:
- Very frequent diarrhea (>6 times/day)
- Severe belly pain
- Fever, dizziness, or signs of dehydration
These symptoms may require hospitalization to prevent serious complications.
Do not assume diarrhea = flare. Testing matters because the treatments are different. Trust your instincts — if your symptoms feel severe or rapidly worse, seek urgent care.
C. diff testing in patients with IBD
Not all positive C. diff tests mean active infection. Some people with IBD carry C. diff bacteria without it causing illness.
Your health care provider should use two-step testing to confirm whether C. diff is actually producing toxins and causing symptoms. If you’re told “you tested positive,” it’s reasonable to ask: “Does this mean active infection, or colonization?”
Treatment for C. diff and IBD
If this is your first C. diff diagnosis, it’s important that your health care provider prescribes the correct antibiotic:
- Fidaxomicin: The preferred first treatment for C. diff in people with IBD. It targets C. diff and doesn’t affect your gut microbiota.
- Vancomycin: This is an acceptable alternative if fidaxomicin is unavailable or too expensive.
- Metronidazole should not be used for C. diff in IBD. If prescribed metronidazole for C. diff, ask why — this is no longer recommended for IBD patients.
Probiotics are NOT recommended for patients with C. diff and IBD.
- Probiotics have not been shown to prevent or treat C. diff in people with IBD.
- In some cases, they may even cause harm in immunocompromised patients.
Staying hydrated is important for your care. Be sure to drink enough fluids and consider adding electrolytes to help keep your system balanced.
Continue your IBD treatment
Being diagnosed with C. diff does not automatically mean you must stop your IBD meds.
- Treating C. diff and controlling IBD inflammation at the same time is important.
- Most IBD medications (biologics, immunomodulators, small molecules) are continued, not stopped.
- Stopping your medicines suddenly may cause your symptoms to get worse.
- Steroids may still be used when needed, with careful monitoring.
Recurrent C. diff and IBD
C. diff often comes back — and prevention matters. People with IBD have a higher risk of recurrent C. diff. After even one recurrence of C. diff, patients should be offered microbiome-based therapies shortly after completing a round of antibiotics, including:
- FDA-approved microbiota therapies, such as fecal microbiota, live-jslm, fecal microbiota spores, live-brpk
- Fecal microbiota transplantation (FMT), when available.
If you’ve had C. diff before and symptoms return, ask early about options to prevent recurrence, not just treat another infection.
Good hygiene and follow-up reduce risk
- Handwashing with soap and water (not just sanitizer) is key, especially after using or cleaning the bathroom and before eating.
- Try to use a separate bathroom if you have diarrhea.
- If using a shared bathroom, disinfect high-touch bathroom surfaces with bleach-based products.
- Review these C. diff cleaning instructions for more information.
- Routine “test of cure” stool tests are not needed unless symptoms continue.
- Close follow-up is important to catch recurrence or ongoing IBD activity early, so be sure to keep in close contact with your health care providers.
Reviewed by

Sahil Khanna, MBBS, MS
Professor of medicine, Mayo Clinic, Rochester, MN

Jana G. Al Hashash, MD, MS
Associate professor of medicine, Mayo Clinic, Jacksonville, FL
Chair, AGA Clinical Practice Updates Committee
April 2026