What is an ostomy?
An ostomy is an opening in your stomach that is made by surgery to let solid or liquid waste leave your body. People with some gastrointestinal (sometimes called GI; also known as the digestive system) conditions, like inflammatory bowel disease (IBD), colorectal cancer, diverticular disease, or intestinal trauma or tear might need an ostomy.
With a gastrointestinal ostomy, solid waste (stool, feces or poop) is changed from its usual path because some parts of your digestive system are not working the right way. An ostomy can be temporary (for a short time) or permanent (forever).
If you need an ostomy, you’re not alone – about 750,000 Americans live with an ostomy and 130,000 new ostomy surgeries happen in the U.S. each year.
What is a stoma?
The opening made by ostomy surgery is called a stoma. The stoma will be made on your stomach and will be dark pink in color. A pouch or bag is worn tightly over the stoma to collect stool. The bag is emptied a few times a day and a new bag is put on every few days.
What are the different types of ostomies?
Colostomy
- Most common type of stoma made from a part of the colon
- Output can be easier to manage with formed stools
- Often needs to be emptied once a day
Ileostomy
- Made from the end of the small intestine (terminal ileum) close to the muscle between your small intestine and colon (ileocecal valve)
- Easier to create and undo
- May cause more dehydration (when your body does not have the fluids it needs) and skin pain, swelling or itchiness
- Output is more liquid and often needs to be emptied 3-4 times a day
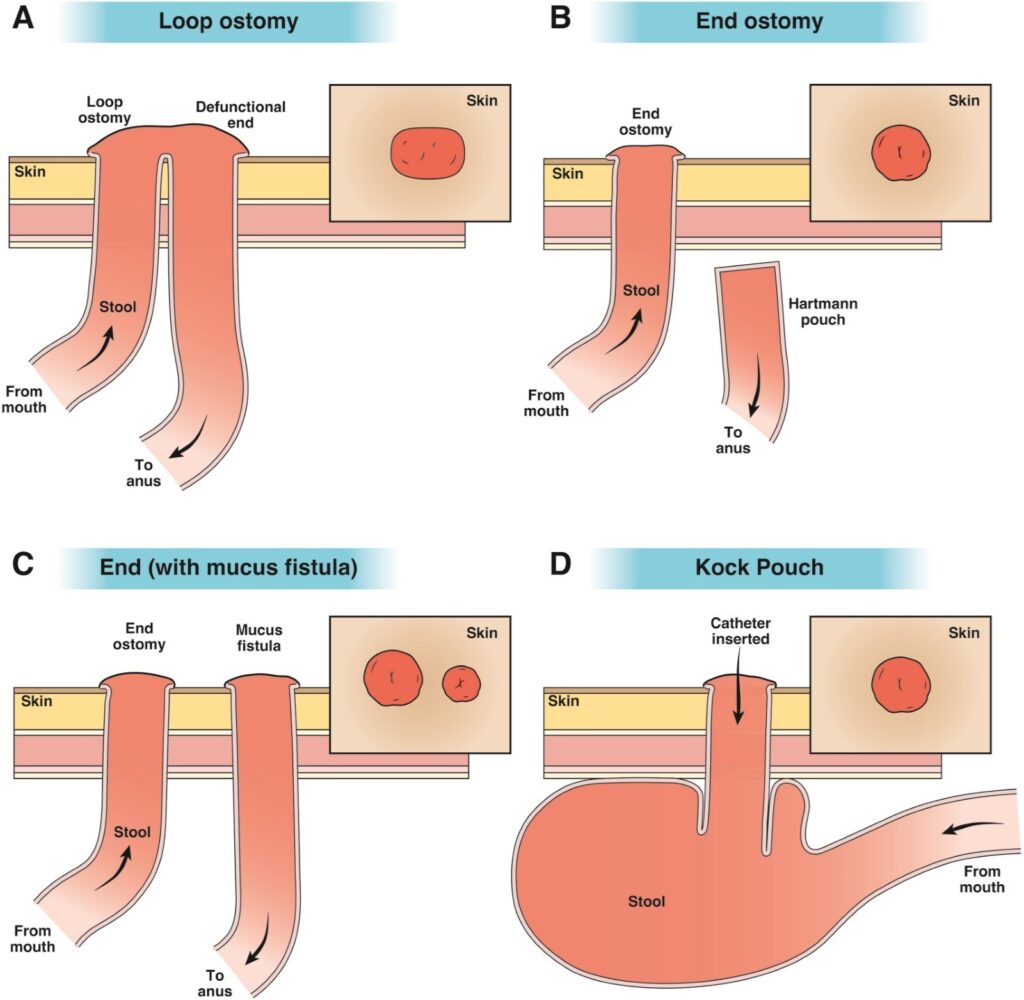
End ostomy
- Made when the part of the intestine that is causing problems is removed, and the closest healthy end of the intestine becomes the stoma. The rest of the intestine stays in the belly.
- The easiest type of stoma for patients to use a pouch
- Most often used in patients who need stomas for the rest of their life
Loop ostomy
- Made by bringing a nonstop piece of intestine through the belly wall leaving two intestinal openings side by side
- Often used when a short-term diversion is needed to keep stool out of a certain area of your intestine
- It’s easy to make and undo
Continent ileostomy
- Also known as the Kock pouch or the Barnett Continent Intestinal Reservoir
- A pouch is made inside your intestine that stops stool from leaving your body on its own
- A tube called a catheter is used to empty stool through your ostomy
- This is not a common ostomy since it can cause a lot of complications or problems
Complications with ostomies
Short term complications
Short term complications can include high ostomy output soon after surgery, as well as:
This is when your body does not have the fluids it needs. You might need to get fluids intravenously, into your veins.
This can because of obesity, where and how the stoma was created, very liquid output, or if your stoma is laying flat on your skin.
This is when your stoma doesn’t stick out and is laying flat with your skin or looks like it has sunk below your skin.
Long term complications
Long term complications can include skin problems around your stoma such as itching, redness or rash, as well as:
This occurs when your ostomy output is more than what you’re drinking, which can lead to dehydration, when your body does not have the fluids it needs, that lasts longer than 3 weeks or starts more than 3 weeks after surgery.
This happens when part of your intestines pushes through the stomach.
- This is when your stoma seems longer and sticks out from your body more than normal.
- Between 5 and 10 out of 100 people will have a stomal prolapse.
Always talk to your health care provider if you have any problems.
Treatment strategies for high ostomy output
| Type of treatment | Examples |
|---|---|
|
Bulking agents |
Pysllium fiber Guar gum Marshmallows |
|
Antimotility agents |
Loperamide Diphenoxylate and atropine Codeine Tincture of opium |
|
Antisecretory agents |
Proton pump inhibitors/H2 agonists Somatostatin analogues (ie, octreotide) |
|
Anti-inflammatory agents (if resulting from recurrent Crohn’s disease) |
Consultation with IBD specialist |
|
Adaptation-promoting agents |
GLP-2 analogues (teduclutide, elsiglutide, glepaglutide, apraglutide) |
|
Surgical |
Reversal of the ostomy with restoration of intestinal continuity when possible |
Other considerations
You might have some concerns about having an ostomy and how it will affect your life. Worries about your ostomy leaking; how and if it will smell; how to talk to your partners, family and friends; if you will need to wear different clothes; romantic intimacy; travel; and trouble with self-care are all normal. Talk to your health care provider and possibly a mental health professional about your fears before and after your surgery. Also visit My IBD Life for more information about some of your concerns.
Before the surgery, ask your health care provider to show you where your ostomy will be and how you should take care of it. They will tell you what to expect from living with an ostomy, such as how to take care of the output, how to take care of your pouch and other appliances, and what to do if something does not seem right.
Talk to your health care provider about any concerns or worries you have.
Resources for education and support
Hear from Alexis Sherman, RN, BSN, CWOCN
"I have lived with an ostomy since the age of 10 and it has allowed me to do so much that I was unable to do before because I was too sick. It takes time to adjust, to not only the physical changes but the mental and emotional ones too. Although it may feel like a burden in the beginning it should not stop you from doing anything. Find the system that works for you to allow you to do the things you love."
Last updated: August 2024

Folasade (Fola) Popoola May
MD, PhD, MPhil,
Assistant professor of medicine, University of California, Los Angeles (UCLA), Health
February 2021